We use cookies to improve your website experience. To learn about our use of cookies and how you can manage your cookie settings, please see our Cookie Policy. By continuing to use the website, you consent to our use of cookies.
Medtech Insight is part of Pharma Intelligence UK Limited
This site is operated by Pharma Intelligence UK Limited, a company registered in England and Wales with company number 13787459 whose registered office is 5 Howick Place, London SW1P 1WG. The Pharma Intelligence group is owned by Caerus Topco S.à r.l. and all copyright resides with the group.
This copy is for your personal, non-commercial use. For high-quality copies or electronic reprints for distribution to colleagues or customers, please call +44 (0) 20 3377 3183
In a deep-dive sit-down interview with Medtech Insight, ALung Technologies CEO Pete DeComo dishes on US FDA's Breakthrough Devices Program and explains why his firm's novel artificial lung device, Hemolung, is worthy of traveling the expedited pathway to agency approval. DeComo also details two pivotal Hemolung clinical trials in the US and UK, and explains why Hemolung isn't marketing the device for commercial use despite being approved in 36 countries outside the US. He also talks about a future portable version of Hemolung, but noted that's not where ALung is focused right now. "Our first task is that first-generation technology – to get it to market, make it the standard-of-care, and then, if you are successful with all of that, you can do all of those wonderful other things as it relates to portability and wearability," DeComo says.
When ALung Technologies Inc. was selected in 2015 by US FDA to participate in the agency's Expedited Access Pathway program for its novel Hemolung device, the firm wasn't necessarily sure what it was getting itself into.
"For the FDA and ALung, it was, 'We’re not sure about this, how is this going to work?'" ALung CEO Pete DeComo said. "We would sometimes ask the FDA, and they would say, 'We don’t know, we’re going to work through it with you.' But I think we’ve gotten to a comfort level with that in terms of our working relationship with the FDA, which has learned along the way and has modified things within its program."
The initiative is an accelerated development pathway for devices that FDA finds could provide a more effective treatment or diagnosis of life-threatening or irreversibly debilitating diseases or conditions, addressing an unmet need. ALung's Hemolung – essentially an artificial lung – meets those qualifications.
A technology developed at the University of Pittsburgh's McGowan Institute for Regenerative Medicine, Hemolung is "different than any other artificial lung technology that exists in the world," DeComo said. "We're the only company that has developed an integrated system that has not only a blood-movement system, but the artificial lung contained within it as well."
Pete DeComo with Hemolung devices in ALung's Pittsburgh headquarters
Source: Shawn M. Schmitt
The device "is designed to be simple, safe and effective. Other technologies that are out there aren’t nearly as elegant in terms of simplicity and safety and effectiveness, as ours is," DeComo added. "It's the only artificial technology designed for extracorporeal CO2 removal, that has been conceived, designed and manufactured from the ground up to do what it does."
Put simply, Hemolung removes from the blood dangerous CO2, much like a kidney dialysis machine takes unwanted waste products out of the blood and places filtered blood back inside the body.
And DeComo knows a thing or two about kidney dialysis devices: He founded Renal Solutions Inc. in 2000 and served as that company's CEO until he left in December 2008 to join ALung. (Fresenius Medical Care AG & Co. acquired Renal Solutions in late 2007.) (Also see "Fresenius Acquires Renal Solutions, Next-Gen Home Dialysis Technology" - Medtech Insight, 3 Dec, 2007.)
"We often joke that ALung is one of the oldest early-stage start-up companies in the City of Pittsburgh," DeComo said. Hemolung "was conceived around 1997/1998, began development and was spun out of the University of Pittsburgh, and ALung was formed around 2000." (See sidebar story, "Life Sciences Greenhouse Plants Medtech Seeds In Pittsburgh," below.)
Hemolung "is typical of complex medical devices and how long it takes to get a technology like this developed and through the regulatory pathway. And it's quite an expensive prospect, as well, to do that," he said. "We've raised a significant amount of money to develop this technology and take it two pivotal trials. It is quite expensive. I won't say how much, but it's a significant amount of money."
HemolungSource: ALung Technologies Inc.
In the US, Hemolung is the subject of the ongoing VENT-AVOID Trial.
"This landmark pivotal trial studies AECOPD, or acute exacerbation of chronic obstructive cardiopulmonary disease," DeComo said. "These are patients who have a progressive disease like emphysema and chronic bronchitis. These are patients who progressively get worse, and typically in their end stage they oftentimes get bacterial or viral lung infections, especially in the flu season. They are admitted to the hospital, and oftentimes they get the breathing tube down their airway, which is called intubation, and they are put on a mechanical ventilator."
Hemolung "is used to either avoid that entire progression or, if they do need the ventilator, to get them off the ventilator sooner, and get that tube out of their airway and get them back to their normal activities of daily living," he said.
VENT-AVOID began in January 2018 and involves 30 trial sites, enrolling between 300 and 600 patients.
Aside from the US trial, "we've treated six patients in the United States on an emergency basis. The FDA permits you to use [a non-approved device] when there are no viable options for these patients, and death is imminent," DeComo said.
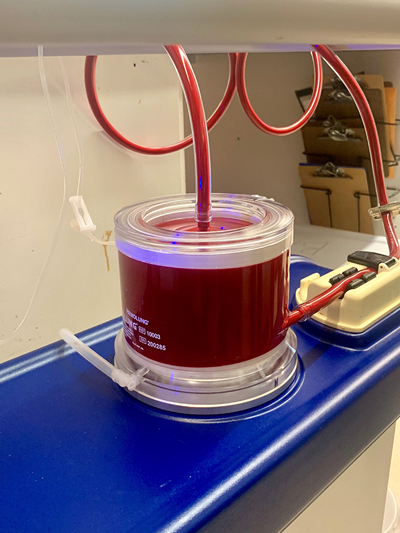
Hemolung's circular cartridge filtering bovine blood during a demonstration
Source: Shawn M. Schmitt
And in the UK, ALung is running the REST Trial, which recently reached 25% enrollment with 280 patients.
"We sell commercially in the United Kingdom, but our primary emphasis is this pivotal trial," DeComo said. "It's studying acute respiratory distress syndrome. These are patients that, for one reason or another – typically due to trauma – their lungs have failed, and our device is used to protect the lungs and get them off the ventilator sooner. It's the largest trial ever done on extracorporeal lung support, where we take blood out of the body, treat it, and put it back into the body."
The REST Trial will eventually enroll 1,120 patients and will likely take five to seven years to complete.
Although Hemolung is approved in 36 countries outside the US, "we're not commercializing in those countries," DeComo said, noting that the company is focusing all its energy on those two pivotal trials.
DeComo declined to estimate the number of lives saved by Hemolung to date, "but I can tell you we're approaching 900 patients that we treated worldwide."
In a deep-dive interview Oct. 16 at ALung headquarters in Pittsburgh, DeComo and Scott Morley, the firm's senior VP of marketing development, spoke with Medtech Insight about Hemolung, clinical trial hurdles and FDA's slowly burgeoning Breakthrough Devices Program.
Medtech Insight: Being a breakthrough device is obviously one of the reasons why Hemolung went through the Expedited Access Pathway, which of course is now called the Breakthrough Devices Program. Tell me about your experience with that program.
Pete DeComo: Relationships with the FDA and the approach of the FDA goes in peaks and valleys. It got very bad about 10 years ago; it started to be very cumbersome to get a device through the FDA pre-market process. And there was a lot of turnover within the FDA. We’re not even sure if the reviewers we were working with understood what they were supposed to be doing within the FDA. Oftentimes when you have a long career in this industry, you go through periods like that with the regulatory bodies.
Then something happens, it reverses, and the industry complains. There are a lot of lobbyists that work with the FDA to try to turn things around. About three years ago, the FDA became much more collaborative, much more compromising with its approach to getting devices approved. One of the challenges that we have with our Hemolung device is that it is a class III device, which is considered to be the highest-risk device. It requires a pre-market approval process in order to get regulatory approval.
What is unfortunate about our device is that we can’t use other extracorporeal devices as a predicate. Kidney dialysis, for example, is a much more complicated process, and devices for that are usually class II. Yet in kidney dialysis, not only do you remove toxins and solutes and things like that, but you have to do electrolyte balance, fluid balance, all of that. It’s a very complex process, and it’s the industry I came from before I came to ALung [in 2009], so I understand it well. MT043493
In ALung’s case, while we do remove blood, treat it, and put it back, it’s a very simple process because all we are doing is gas exchange. Yet, we are classified as a class III, which makes life much more complicated than it would be for a kidney dialysis machine.
Why is it that a kidney device is class II, but Hemolung is class III?
DeComo: In kidney dialysis, those devices have been on the market for quite a long time. Many have been approved. In the development of a kidney dialysis machine or technology, because there are other devices in the market that are approved, even though your device is a little bit different, you can claim substantial equivalency to those devices. We can’t claim substantial equivalency to anything because there is no device that’s gone before Hemolung that has been approved by the FDA that is similar.
Scott Morley: Thus, there is no classification, according to federal regulations. The long history on extracorporeal membrane oxygenation [ECMO] products is that, since the 1970s, when they first came out, they’ve all been approved only for short-term use for no more than six hours under the class II cardiopulmonary bypass controls. It wasn’t until about two years ago that the FDA created a new classification of ECMO products for long-term support. (Also see "Oxygenation Circuit Devices Find A Class II Home With FDA" - Medtech Insight, 11 Feb, 2016.) They limited that indication to something very specific, which is essentially the current ECMO – severe refractory, life-threatening oxygenation issues. That is a different indication than what we are pursuing, which is a larger, broader market for carbon dioxide retention in patients with acute chronic respiratory failure.
DeComo: All of those devices that were used for six hours were typically used in the operating room for heart-lung bypass procedures. But ECMO, which is a similar process to what we do, has been used for years to treat patients that have significant oxygenation needs, or even carbon dioxide retention. But it’s all been off-label use. As a result, as I said earlier, there is no predicate that we can claim substantial equivalency to, and therefore that throws us into a class III PMA-approval process.
Morley: But to get back to your original question, which was how the Breakthrough Devices Program is going – the Breakthrough process has been a really interesting thing for us, and very beneficial. The agency has been very collaborative, very interactive. I almost was going to say accommodating, but that’s maybe not quite right.
DeComo: That’s overstating it.
Morley: Yes, but they're being interactive and collaborative – true professionals and an excellent team, very scientifically sound and willing to collaborate and try to understand our perspective on things.
DeComo: The other thing I would mention is that our team at the FDA has been very stable; there's been very little turnover, if any at all. Our section chief understands our technology and has been working with us for a number of years. That’s all been great, and we hope it stays that way.
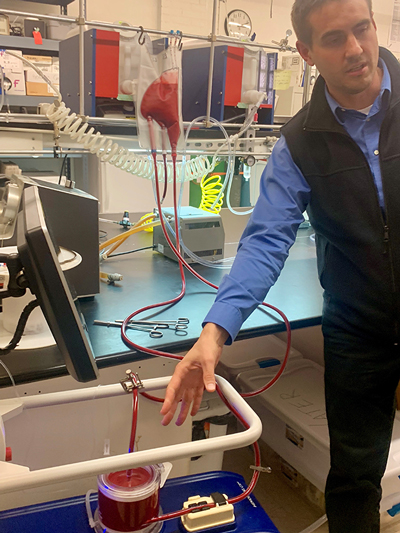
Scott Morley, ALung's senior VP of marketing development, shows off the Hemolung
Source: Shawn M. Schmitt
You spoke in glowing terms about the Breakthrough Devices Program. But is there anything that you wish FDA would tweak about the program?
DeComo: We’re caught between a rock and a hard place because the protocol that we have approved by the FDA to do our trial is a biproduct of six to seven years of discussions with the FDA to get to a point where they were comfortable enough with all of our testing – our in vitro and our animal testing, et cetera – and with the trial protocol to give us approval to do our trial. The mentality of the FDA relative to trial structure six to seven years ago is very different than the mentality of the current FDA relative to the trial structure. Along that six- to seven-year pathway of getting to approval from that trial, what we ended up with was a trial that is very complex, very costly and very cumbersome. As a result, it has taken us a significant amount of time to get trial sites through the contracting process. Now that they are able to screen and enroll patients, what we are finding is that the trial protocol relative to inclusion and exclusion criteria is overly burdensome. The inclusion and exclusion criteria are very tight. With the change in the mentality by the FDA, we have now gone back to them and we are working with them collaboratively to modify the trial protocol to make it less cumbersome but still scientifically meaningful. The FDA is currently reviewing our recommendations to doing that. That is one thing we want to change and need to change. The FDA has been very receptive of our recommendations. They are in the review process right now, so I can’t comment on what the outcome of that will be. We are optimistic that the current FDA and its methodologies, its way of thinking, will be to our benefit as we come out the other end of this review process on the revised protocol changes.
And there are two trials for Hemolung – one in the US and one in the UK.
DeComo: Correct. The US trial is called the VENT-AVOID Trial. We'll have 30 sites by the end of the month [October 2018]. We’re allowed up to 40 sites in our protocol. We will be 30 sites through this flu season, but ultimately we will get to 40. We’re stopping at 30 because the other 10 would take time and effort, and they wouldn’t be ready for this flu season. We’ll get them up and running after we get these 30 proficient at what they are doing.
Why is it so important to do the trials during flu season?
DeComo: In the colder winter months is typically when the flu happens, starting around September, October and through March, April. What happens in the colder months is, you have a higher viral load in the atmosphere. The viruses can live in that type of environment, and patients with COPD [chronic obstructive pulmonary disease] are more susceptible to lung infections in the colder winter months.
"Our routine interaction with the FDA is weekly. That never happened before," Pete DeComo says of FDA's Breakthrough Devices Program.
And your trial for Hemolung in the UK is…
DeComo: The UK REST Trial. That trial is for a different indication for use. In the US the indication for use is for acute exacerbation of COPD. But in the UK REST Trial, it is for ARDS – acute respiratory distress syndrome. COPD is a chronic disease. You have it, and you get progressively worse over time. With ARDS, you typically don’t have a respiratory disease, but you have acute respiratory failure for some reason. It could be smoke inhalation in a fire; it could be blunt-force trauma to the chest in a car accident; it could be vomiting and aspirating your gastric contents into your lungs and burning your lungs. A variety of reasons cause ARDS, including severe flu, as well. It’s a different indication with a different trial structure and a different endpoint.
How many sites for the UK REST Trial?
DeComo: Around 40 also.
Endpoints for the trials – timeframes?
DeComo: Because of the seasonal nature of the flu, we think it will take us two flu seasons, this one being our first. Now, that doesn’t mean we don’t enroll patients through the summer months; it’s just less frequent because it is warmer. Then we'll go into the 2019-2020 flu season, and hopefully we are ramping our enrollments along the way as our clinical sites become more proficient. Yes, enrollment will slow in the summer months, but when you get into the second flu season, things should all be rip-roaring, ready to go. So, right now we are projecting two flu seasons. We should finish enrollment in the trial, if all goes well, sometime at the end of the first quarter or early second quarter of 2020. And then we’ll crunch the data and submit all that to the FDA for approval.
Are you in contact with any other companies that are also going through the Breakthrough Devices Program process?
DeComo: Yes, we’ve talked to a few, but not recently.
I didn’t know if maybe you talked to others and said, "Hey, we're having the same issues, so let’s…"
DeComo: No, to be frank about it. The reason we don’t seek out those kinds of companies, and it goes to my comment earlier, is there is no other technology like [Hemolung] in the Breakthrough program, to our knowledge, and no other competitive technologies are pursuing the Breakthrough program.
The Breakthrough program requires monitoring in the post-market phase. Obviously, you are not post-market. So, FDA doesn't want anything from you on that end yet.
DeComo: Not yet, no.
But when you do get to that point, what kind of data do you think you’d be collecting?
DeComo: We’re familiar with post-market surveillance programs. We had to do the same thing in Europe. I don’t want to say they are not difficult to do, but you just need to put structure and function in place in order to do them. But to your point, from what we can see with the FDA is that part of their changing mentality is to shift the burden of demonstrating safety and efficacy to the post-market phase through a surveillance program like that. They are much more accepting today of real-world data, including European data, where they weren’t so receptive to accepting real-world data, European data, publications, to substantiate safety and efficacy, as they are today. What we’re doing with the FDA is talking to them about all of those things, how that can work to our benefit to reduce the burdensome nature of our protocol, and providing in the future real-world data information to them that says, let's shift some of this to the post-market approval stage, versus having to do this large, scientifically-based pivotal trial type protocol that requires hundreds and hundreds of patients to show safety and efficacy. Again, we don’t know the outcome of those discussions yet, but we are working with the FDA on those things.
"We can’t keep our technology on the market commercially and try to drive sales, while at the same time funding two large, landmark pivotal trials," DeComo says.
Have you noticed any difference in the program since FDA shifted from the Expedited Access Pathway to the Breakthrough Devices Program?
DeComo: No. As I said, the EAP program was meant, on the FDA side, to assign you a team leader and a team that works with you through the process. Our routine interaction with the FDA is weekly. That never happened before [the program]. We are talking to the FDA weekly, there are e-mail exchanges going on, exchanges of information going on continuously as it relates to the program and our clinical trial. That’s refreshing, because prior to that you didn’t know when you were going to have communication with the FDA, or about what. They know how we think. They now have a comfort level with the quality of work we do. We have no discomfort with speaking to them whatsoever. They’ll shoot us questions, we’ll shoot them answers. We get through things relatively quickly.
You talk weekly? Do things change that much that you need to talk to FDA weekly? Or are there some weeks that you say, "There's nothing to talk about"?
DeComo: No. There is always something to talk about. For example, our protocol is a PMA modular protocol. What that means is, as we go through our clinical trial, we submit in modular format to the FDA as we go through it. In other words, you submit module one and you go through a review process with the FDA. There is a Q&A period, and you go back and forth on all that stuff. Once you get through module one, as you progress, you then submit module two. Then you submit module three, and it’s a progressive approach to your total application. When you finally get to module four, when you are submitting clinical data, you’ve got modules one through three behind you. You ask what we talk about? Well, module one has been submitted already, and FDA is shooting us questions. We get on the phone with them weekly and we go over those questions or we submit back to them in writing. That’s just one example of one of the things you constantly have to talk about. And we’ve had numerous phone calls with the FDA, talking about what our current status is with the trials, what challenges are we facing, what would we change if we could change it. That all results in work that we do to formulate a formal submission to the FDA on what we want those changes to be. Then we go through a Q&A period with the FDA on that. There is always something to talk about with the FDA.
You said Hemolung is approved in 36 countries, and that you're selling in the UK. Correct?
DeComo: Our main emphasis is not commercialization right now. Our main emphasis is on our two landmark pivotal trials. When I said we are selling in the UK, I meant [that Hemolung is] in approximately 40 sites in the UK for the UK REST Trial. If those sites have a patient that does not meet the criteria of the clinical trial, but they believe they need our therapy, that would be a commercial patient, which they would pay us for. Most of our business in Europe is in the UK and only for the clinical trial. We do generate a little revenue, but that is not our emphasis at all.
If Hemolung is approved in so many countries, why aren’t you commercial?
DeComo: We did attempt to do that initially, to commercialize in Europe. What we heard from the market was that it loved the technology and it thinks the data is compelling – but the data is not validated. So, what we did in 2015 was say, "OK, market, we hear you. But we can’t do both. We can’t keep our technology on the market commercially and try to drive sales, while at the same time funding two large, landmark pivotal trials. You are saying you need this data, so we are going to go get it." Right now, we are the only technology and the only company in the world doing pivotal trials of this magnitude. What that means to us is, if we are successful validating the safety and efficacy of our technology and this therapy, we have basically created a barrier to entry to anybody who might follow us. In the United States, you cannot claim substantial equivalency to a PMA trial technology. You have to go do that yourself. No other company and no other technology have chosen to do that. I have to give our board and our investors a great deal of credit in terms of supporting the company and allowing us to do those pivotal trials. There is a lot of risk associated with that, because it takes a lot of money to support these types of trials.
"Our first task is that first-generation technology – to get it to market, make it the standard-of-care, and then, if you are successful with all of that, you can do all of those wonderful other things as it relates to portability and wearability," DeComo says.
I understand ALung is looking to develop a portable version of the Hemolung. Could you talk a bit about what you're planning?
DeComo: [Hemolung] is primarily designed for intensive-care unit use. However, being somebody who has come from the home-care environment, a device of that size with that footprint could be easily used at home as well, if the home market existed. But, if made for military use, for example, a portable version could be used in a helicopter for transport, or in an ambulance for transport. It could be used with the same catheters. In a wearable lung, what you want is a lung that is highly efficient; smaller of course, it could be in a belt or a backpack. The vascular access – in the Hemolung, we are using catheters in the jugular or catheters in the femoral – in an ambulatory situation, it could be implanted into a vessel. Not the lung itself, but the vascular access could be into a vessel surgically. Or, as in the case of kidney dialysis, you could use peripheral vascular access. In kidney dialysis, they use a shunt or implantable ports right under the skin. They also use a buttonhole technique, which is a mature tract right into the vessel. You just put a blunt-edge needle right into the shunt or the fistula. Those would be things that would be developed in the future to support a portable lung. We have wearable, portable, artificial lungs on the bench in development today at our partner organization at [the University of Pittsburgh's] McGowan Institute. Those technologies are in the R&D phase and eventually will move over to us in the commercial-development phase. But that’s a whole new project. Typically, in the start-up world, we try to be laser-focused on our first task. Our first task is that first-generation technology – to get it to market, make it the standard-of-care, and then, if you are successful with all of that, you can do all of those wonderful other things as it relates to portability and wearability. Then you’ll have revenue, you’ll have profitability, and/or you’ll be able to attract significant investment dollars to do those kinds of things.
Ask the Analyst is free for subscribers. Submit your question and one of our analysts will be in touch.
Your question has been successfully sent to the email address below and we will get back as soon as possible. my@email.address.
All fields are required.
MT123493
Email Article
All set! This article has been sent to my@email.address.
All fields are required. For multiple recipients, separate email addresses with a semicolon.
Please Note: Only individuals with an active subscription will be able to access the full article. All other readers will be directed to the abstract and would need to subscribe.